Nature is a patient, not a machine: Looking at stream restoration through the medical lens
August 27, 2018
Select your region to visit a Stantec regional site, or visit our Locations Hub on our Global site where you can learn more about Stantec in your local area.
", "languageSelectorImage": { "imageLarge": "\/content\/dam\/stantec\/images\/Icons\/Map.svg" }, "globalRegion": { "name": "Global", "regionTag": "localization:global", "description": "", "languages": [ { "langCode": "en", "name": "English", "pathLink": { "url": "en" }, "active": "true" }, { "langCode": "fr", "name": "Français", "pathLink": { "url": "fr" }, "active": "false" } ] }, "regionLanguages": [ { "regionTag": "localization:china", "name": "China", "description": "", "languages": [ { "langCode": "en", "name": "English", "pathLink": { "url": "cn" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:italy", "name": "Italy", "description": "", "languages": [ { "langCode": "it", "name": "Italiano", "pathLink": { "url": "it" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:latin\u002Damerica", "name": "Latin America", "description": "", "languages": [ { "langCode": "es", "name": "Español", "pathLink": { "url": "es" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:netherlands", "name": "Netherlands", "description": "", "languages": [ { "langCode": "nl", "name": "Nederlands", "pathLink": { "url": "nl" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:taiwan", "name": "Taiwan", "description": "", "languages": [ { "langCode": "zh_tw", "name": "繁體中文", "pathLink": { "url": "zh_tw" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:turkey", "name": "Turkiye", "description": "", "languages": [ { "langCode": "tr", "name": "Türkçe", "pathLink": { "url": "tr" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] } ], "originPath": "/content/stantec/en/ideas/content/blog/2018/nature-is-a-patient-not-a-machine-looking-at-stream-restoration-through-the-medical-lens.html" }, "locationSelector": { "locationInformationText": "We\x27ve detected you are located in", "locationDropdownText": "Please select your location", "changeLocationText": " Change location", "locationSaveText": " Save location", "learnMoreText": "Learn how we use this information", "regions": [ { "tag": { "tagID": "localization:africa" }, "title": "Africa" }, { "tag": { "tagID": "localization:australia" }, "title": "Australia" }, { "tag": { "tagID": "localization:belgium" }, "title": "Belgium" }, { "tag": { "tagID": "localization:caribbean" }, "title": "Caribbean" }, { "tag": { "tagID": "localization:china" }, "title": "China" }, { "tag": { "tagID": "localization:czech\u002Drepublic" }, "title": "Czech Republic" }, { "tag": { "tagID": "localization:germany" }, "title": "Germany" }, { "tag": { "tagID": "localization:global" }, "title": "Global" }, { "tag": { "tagID": "localization:india" }, "title": "India" }, { "tag": { "tagID": "localization:italy" }, "title": "Italy" }, { "tag": { "tagID": "localization:latin\u002Damerica" }, "title": "Latin America" }, { "tag": { "tagID": "localization:middle\u002Deast" }, "title": "Middle East" }, { "tag": { "tagID": "localization:netherlands" }, "title": "Netherlands" }, { "tag": { "tagID": "localization:new\u002Dzealand" }, "title": "New Zealand" }, { "tag": { "tagID": "localization:north\u002Damerica" }, "title": "North America" }, { "tag": { "tagID": "localization:slovakia" }, "title": "Slovakia" }, { "tag": { "tagID": "localization:taiwan" }, "title": "Taiwan" }, { "tag": { "tagID": "localization:turkey" }, "title": "Turkiye" }, { "tag": { "tagID": "localization:united\u002Dkingdom" }, "title": "United Kingdom" } ], "currentRegion": "Global", "learnMoreLink": { "url": "\/en\/copyright.html", "target": "" } }, "searchBar": { "searchPageLink": { "url": "\/en\/search.html" }, "labels": { "searchInputLabel": "Search Input", "searchBarPlaceholder": "What are you looking for?", "closeButton": "Close Button" } }, "languageSelectorModal": { "languageSelectorTitle": "Language \/ Region", "languageSelectorDescription": "Select your region to visit a Stantec regional site, or visit our Locations Hub on our Global site where you can learn more about Stantec in your local area.
", "languageSelectorImage": { "imageLarge": "\/content\/dam\/stantec\/images\/Icons\/Map.svg", "altText": " World map" }, "globalRegion": { "name": "Global", "regionTag": "localization:global", "description": "", "languages": [ { "langCode": "en", "name": "English", "pathLink": { "url": "en" }, "active": "true" }, { "langCode": "fr", "name": "Français", "pathLink": { "url": "fr" }, "active": "false" } ] }, "regionLanguages": [ { "regionTag": "localization:china", "name": "China", "description": "", "languages": [ { "langCode": "en", "name": "English", "pathLink": { "url": "cn" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:italy", "name": "Italy", "description": "", "languages": [ { "langCode": "it", "name": "Italiano", "pathLink": { "url": "it" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:latin\u002Damerica", "name": "Latin America", "description": "", "languages": [ { "langCode": "es", "name": "Español", "pathLink": { "url": "es" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:netherlands", "name": "Netherlands", "description": "", "languages": [ { "langCode": "nl", "name": "Nederlands", "pathLink": { "url": "nl" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:taiwan", "name": "Taiwan", "description": "", "languages": [ { "langCode": "zh_tw", "name": "繁體中文", "pathLink": { "url": "zh_tw" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] }, { "regionTag": "localization:turkey", "name": "Turkiye", "description": "", "languages": [ { "langCode": "tr", "name": "Türkçe", "pathLink": { "url": "tr" }, "active": "false" }, { "langCode": "en", "name": "", "pathLink": { "url": "en" }, "active": "false" } ] } ], "originPath": "/content/stantec/en/ideas/content/blog/2018/nature-is-a-patient-not-a-machine-looking-at-stream-restoration-through-the-medical-lens.html" } }August 27, 2018
We shouldn’t treat natural channel design like any other engineering project
Bad news: you’ve torn a ligament in your knee. Good news: you can have surgery to repair it. You have your pre-consultation with the surgeon, coordinate your ride to and from the hospital, and patiently wait for the day to come. Then you go in on the big day, the surgery is flawlessly performed, you wake up from the anesthetic and … hop right back onto the soccer pitch?
Of course not. You wake up from surgery and embark on months—perhaps years—of rehabilitation until you are “ready to play” again. We all know this, and we all accept it in the medical model.

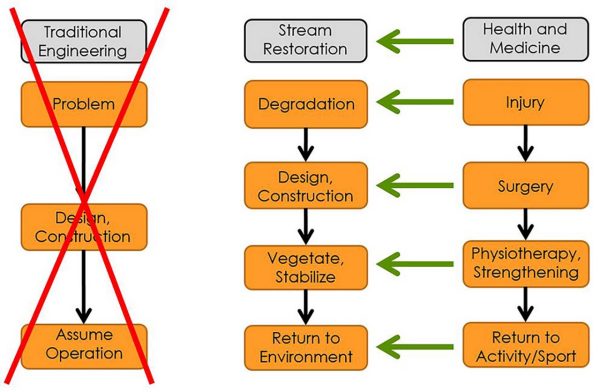
When a watercourse has become degraded, it is analogous to a patient incurring an injury. Author Jeff Muirhead and his team design a natural channel design, just as a surgery is planned. Help the stream recover, and you can return it to activity safely!
Why am I talking about the medical model in a stream restoration blog? Well, let’s compare it to the traditional engineering-construction model that stream restoration projects typically follow.
Let’s consider a watercourse which needs to be restored, realigned, or repaired. A natural channel design (NCD)—which uses the principles of natural watercourses to produce a long-term, sustainable solution—is developed by geomorphologists, biologists, planners, and engineers. Design drawings are finalized and approved, the project is tendered and awarded, and then the big day comes when construction is completed. And then … everyone gets paid and goes home. The project is “finished.” Sound familiar?
The above sequence happens more than we all care to admit in this industry. That traditional engineering-construction model works for many types of projects, including roads, buildings, and electronics. They all are designed to work right away, and it’s assumed that once construction is completed, the product is finished and ready for full implementation.
Unfortunately, NCDs don’t work that way. And I would argue the medical model is a much more appropriate one to follow.
The inspiration for this analogy didn’t come from my own creative volition. It came from the local newspaper in Virden, Manitoba. Back in October 2016, we were amid construction on Brierwood Creek, a channel realignment project in rural southwestern Manitoba. Along came Anne Davison, a local journalist who studied environmental science at Brandon University, who joined us for a site tour and interview. Anne wrote an article on the Brierwood Creek project in the December 2 issue of Empire Advance, the Virden newspaper, and the article included the ingenious title “Surgery on Brierwood Creek.”
Anne was onto something.
When a watercourse has become degraded, it is analogous to a patient incurring an injury. We design a NCD, just as a surgery is planned. The construction phase is just like the surgery phase, and to an observer, a construction site truly does look like surgery. Water is diverted around the construction site, dewatering and erosion control measures are scattered all over, machines are moving in multiple directions, and sod, plants, and topsoil are stripped back.
Performing construction for natural channel design is like doing surgery on the environment.
It’s chaotic. And amidst that chaos, a new, natural channel is constructed, and the site is “sewn” back together with imported material, finished grades, seeding, plantings, and matting.
Under the traditional engineering-construction model, this would represent a finished product. The medical model, on the other hand, recognizes that the patient is in a vulnerable state immediately after surgery and that it will take time and effort to return the patient to activity. That “sewn-up” NCD construction site is similarly vulnerable, and it will take time and informed supervision for the site to recover: grass needs to grow, plants need to take hold, and root structures need to become established below-grade. A road may be ready for 50,000 cars the day after construction, but a stream is not ready for a 50-year flood the day after construction.
The take-home point is this: we shouldn’t treat NCD like any other engineering project. Performing construction for NCD is like doing surgery on the environment. And if we want a stream that is “ready to play” one day, we need to help it recover—just like you would with a post-operative patient wanting to play soccer again one day.

A road may be ready for 50,000 cars the day after construction, but a stream is not ready for a 50-year flood the day after construction.
There is no chance that a surgeon would send their patient back to the soccer pitch the day after knee surgery. If they did, they would lose their license. As river professionals, we shouldn’t send our NCDs back to nature without helping the river recover first.
If we accept this analogy to the medical model and shift our thinking, there are several logical questions that follow. Those questions involve monitoring, contract structures, payment and warranties, among others.
