Hospital HVAC case study: How a new isolation room helps protect vulnerable patients
September 18, 2023
September 18, 2023
Westmead Children’s Hospital needed new isolation rooms to prevent the spread of infection for the safety of immunosuppressed patients
At the Children’s Hospital at Westmead in Sydney there are children in the acute services building who need extra special care—they’re about to get an organ transplant. Naturally, their bodies will try to reject transplanted organs. It’s the immune system response: attack anything unfamiliar. So to tame the body into accepting the new organ, the patient is given immunosuppressing drugs that block the immune system’s response completely. The drugs, naturally, make the child much more vulnerable to infections.
The staff in Westmead’s Paediatric Acute Services asked: How can we protect patients who are infectious or vulnerable and susceptible to further infections? And protect the staff who are treating them? If a transplant patient, whose immune system has been shut down, catches a highly contagious airborne disease like measles, where’s a suitable environment to place them?

Vulnerable patients—like an immunosuppressed child awaiting an organ transplant—or patients with confirmed or suspected infectious diseases need to be isolated. It’s a protection for them and others. They’re placed in isolation rooms, which basically provide a barrier to contain airborne pathogens or prevent their entry.
Air conditioning and ventilation systems maintain pressure differentials between the isolation room and adjoining areas. Differential pressure is essentially the difference in pressure between two given points. In this case, it’s the difference in pressure between the room and area outside of the room.
Isolated patients are usually put into one of two isolation rooms—a positive-pressure or a negative-pressure room. Neither option offers the right level of protection for an immunosuppressed, infectious patient.
Normally, immunocompromised patients are placed in positive-pressure isolation rooms that have HEPA (high efficiency particulate absorbing) air filters. This helps reduce the risk of infection to the patient. The air conditioning system works by pushing air out of the room.
If the isolated patient contracts an infectious disease, the air will become contaminated. It will be pushed out of the room into adjoining spaces where staff, visitors and other patients are exposed to the risk of catching the infection too. Thus, the positive pressure isolation room is unsuitable.

Immunosuppressed or immunocompromised patients who are infectious are placed in negative-pressure isolation rooms. This helps reduce the risk of the infection spreading to others. The way this works is that air is drawn into the room, as opposed to being pushed out like we saw in the positive-pressure room. However, if contaminated air gets in, it could worsen the patient’s condition by exposing them to further infection. This could be fatal for someone whose immune system is suppressed. That means the negative-pressure isolation room is also unsuitable.
The Westmead Children’s Hospital Acute Services unit needed a better option. It needed to work for everyone’s safety and health. Our team conducted a deep literature review, assessing Australian, British, American and European guidelines and academic research. We found the solution in the British Health Technical Memorandum, from a supplementary guideline focused on ward isolation rooms.
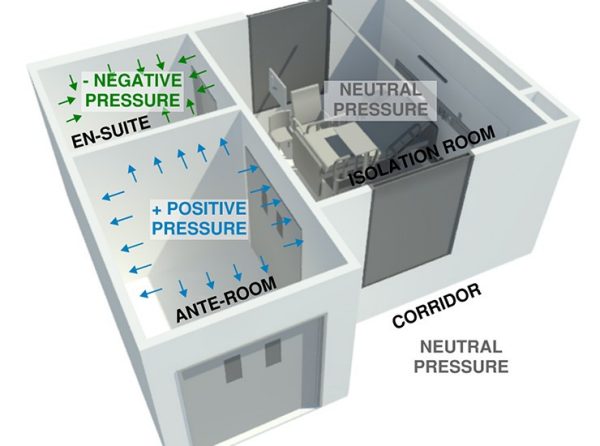
There’s a relatively new isolation room design called a positively pressurised ventilation lobby isolation room (PPVL). The principle of the PPVL is to provide a safe barrier on both sides of the isolation room. It stops airborne infection originating from the isolation room and from the hospital ward.
How can we protect patients who are infectious or vulnerable and susceptible to further infections? And protect the staff who are treating them?
The anteroom is positively pressurised relative to the corridor and bedroom with HEPA filtered air. This arrangement achieves two outcomes. First, it isolates the patient from the ward like a negative isolation room. Second, it also provides protective isolation like a positive isolation room.
The pressure differential between the isolation room and the adjacent corridor is intended to be neutral. This design achieves low air permeability between the isolation room and nearby spaces. Neutral pressure in the isolation room alone offers little protection against air coming in and out through cracks and gaps. Therefore, the performance of the PPVL requires that the room is well sealed.
In a typical PPVL arrangement the air flow in a neutral pressure room is supplemented by seals.
The design was validated by UK-based engineering research company BSRIA. What did they do? They built a full-size physical model including ventilation systems, pressure stabilisers and hospital furniture.
Then they thoroughly tested the design in control and ‘failure’ situations. These included anemometry—the force, speed and direction of airflow—air tightness, ventilation devices, gas and smoke tracing, and heat load. And they measured ventilation patterns, airborne infection risks inside and outside of the PPVL, and the occupants’ thermal comfort.
Remember, the whole point of the isolation room design is protection. It should keep bugs from escaping and risking visitors and staff outside the PPVL. It should also give some protection to the immunosuppressed patients who are in the isolation room.
BSRIA’s testing showed that when all the doors were closed the air leakage from the isolation room to the corridor was at acceptable levels. The ventilation strategy also dilutes the contaminant concentration within the isolation room. In any scenario, healthcare workers must wear personal protection equipment when treating a patient to mitigate the risk of infection.

The Westmead PPVL arrangement includes bed access via an anteroom and sliding doors.
For most Australian healthcare facilities, isolation rooms are usually accessed directly from corridors via double-leaf doors. Beds and equipment are rolled in through these doors. And when there’s a patient in the isolation room, staff access the isolation room via the anteroom. This is a problem for a PPVL suite. The PPVL requires a well-sealed space. Accessing the isolation room directly from a corridor through double doors will defeat the design’s purpose by increasing the potential for leakage.
At Westmead, we had to make a compromise. By reducing the number of PPLV rooms the hospital wanted we could achieve a low-risk design by creating access through the anteroom only. This limited the risk of leakage between the bedroom and the rest of the hospital. We also introduced sliding doors to facilitate bed movement.
Westmead Childrens Hospital Pediatric Services Building is under construction, and the PPLV isolation room will become a reality in Australia in 2024. This type of room is an alternative to the status quo. Its unique features lend itself to the safe treatment of patients undergoing any type of transplant. The next steps are to promote awareness of this configuration and advocate for its inclusion in relevant Australian guidelines.
