Why decarbonizing hospitals smartly is better than electrification for healthcare design
January 18, 2024
January 18, 2024
Decarbonizing hospitals requires meeting peak demand, extra space, and innovative design approaches
There’s a new conversation happening in healthcare today. Driven by new laws, regulations, tariffs, ESG goals, and thought leaders in the industry itself, healthcare institutions are embracing decarbonization to meet 2050 goals for emissions reductions. With the health sector contributing to about 5 percent of global carbon emissions, many of our clients are, quite naturally, anxious to embrace electrification as a shortcut to decarbonizing hospitals. They’re being told to decarbonize now. But often what we hear them asking for isn’t a realistic pathway to hitting their targets. And it’s not achievable on their budget.
As healthcare engineers who have been engaged in finding low-carbon solutions on major projects, we’re not new to decarbonization and its challenges. We have worked on healthcare projects of all scales from small local renovations to large full facility renovations and new construction. The common thread that runs through these projects is a desire to reduce energy consumption and emissions in practical, affordable, and constructable designs. We’re experts in implementing lower-carbon approaches on demanding projects.
We’ve been at the forefront in design and engineering to reduce the energy appetite of healthcare buildings. What was once innovative—design to reduce the energy load, then design to recover as much of the thermal energy as possible, and right size efficient systems—is now a standard approach.

Healthcare facilities are unique—they must be fully operational, all the time. So, the jump to 100 percent electrification of the facility may not be practical.
At the same time, we have a detailed understanding of healthcare’s unique resiliency needs, also known as continuity of operations. When we design facilities, part of the process is knowing that the buildings must operate during catastrophic events, even when they lose their primary power supply. This has implications for electrification.
Electrifying the hospital is not a simple matter. When we get into the nitty gritty, a lot of issues arise—some of which have serious impact on the budget. We believe in a sensible approach to electrification that uses resources wisely. Bridging the knowledge gap with clients around healthcare electrification can give their decarbonization efforts a better chance to succeed.
Here are six aspects of healthcare facility electrification our clients should understand. And we’re also sharing four strategies that are key to smart decarbonization.
Some clients assume that electrification means accessing clean energy. But the electricity we access from the grid is only as clean as the fuel source for that electricity. In many regions, the electricity on the grid comes from fossil fuels. That means it comes with their associated emissions and transmission losses. On a recent project, our analysis showed it would be cleaner to use natural gas than to use electricity for heating because the regional grid was quite dirty.
Eventually, North America will have clean energy and the infrastructure that can handle it. In the meantime, we need to be aware of how clean or dirty the grid is when we make plans to electrify.
On a recent major project, the client asked for a series of features that combined full electrification with high standards for operations. These included:
While each item made sense in isolation, when combined with full electrification they added up to enormous theoretical peak demand. Why?
In healthcare design, we always design for worst-case scenarios, what we sometimes call “Sharknado events.” That’s because hospitals are essential. They need to stay open on the hottest and coldest days of the year, which may coincide with catastrophic events. Thus, we design to meet that theoretical peak demand—for a day that may never come.
The peak load on the coldest day of the year might be double the base load under normal conditions. It is magnified if we design for a pandemic event, which may require operating in 100 percent outside air mode. If we’re switching to 100 percent electrical, that means that the electrical service to the building must be sized to handle peak condition—and the electrical transformer, too. In the winter we may also need to humidify the air. And that requires power. What if we lose primary power supply on site? The back-up system needs to handle the peak load.
So, a building system sized to maintain 40 percent relative humidity on the coldest day of the year, with 100 percent outside air and backup power, has a huge electricity demand. Simply testing that system’s emergency generators weekly might eclipse the carbon savings when compared with a right-sized decarbonization strategy (more on that below).

A sensible approach to electrification in healthcare uses resources wisely. It’s important to bridge the knowledge gap with clients around healthcare electrification and can give their decarbonization efforts a better chance to succeed.
Full or even near full electrification for healthcare also affects the architecture. We need to design larger electrical rooms, bigger risers, and larger clearance zones for it.
Our analysis shows that a large hospital system could require an additional 10 percent of mechanical and electrical room space to electrify. This has huge budget impact for hospitals.
Even efficient hospital systems need a lot of power. While several factors determine the electrical demand for a hospital, the rule of thumb is that going all electric will double the hospital’s need for power from the grid.
Imagine approaching a local municipal power utility and explaining that the new hospital building will need more power than the city itself. In many places, the grid simply doesn’t have the capacity to provide for a fully electrified hospital building, let alone a healthcare campus.
In the field, we have seen owners and operators caught by surprise by the operational consequences of electrification. For example, we have seen non-Stantec built projects where the high level of electric current going through the service panels creates a high arc flash hazard. To service these systems, facility staff need to wear specialized personal protective equipment (PPE), resembling space suits, and receive additional training. This is not something the owner wants to hear about only after the building has been switched on.
Clients are accustomed to paying for the fuel their buildings use. For an electrified building, the billing system is different. They’re charged for the volume of energy used (kWh) as well as a demand charge (kW), which is based on peak demand. The way demand charges are calculated can vary, but it’s usually based on the customer’s peak power consumption over a short time interval. Time of use billing further adds premium costs and complexity to billing estimation.
So, what kind of strategies do we suggest to deal with these issues around hospital decarbonization?
When we talk about electrification, that means designing everything to run on electricity, right? Not necessarily. Does it really make sense to size electrical systems for those very high consumption days? The answer is that an almost-electrified building is often better than true net zero. If we look at a typical graph for electricity demand in hospitals, we spend most of our time in the middle. Consumption only spikes for a few hours or days. And the likelihood of hitting theoretical peak demand is remote.
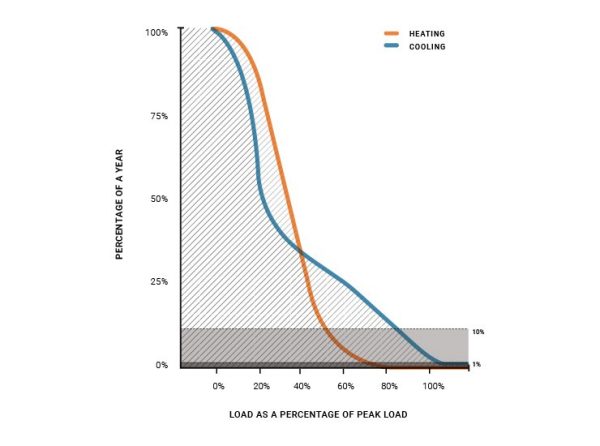
By graphing aggregate data from real healthcare facility projects, we can see that a typical modern North American hospital spends less than 10 percent of the year operating above half the peak heating load. It spends less than 1 percent of the year operating above 70 percent of peak heating load.
Electrified hospitals will still require fossil fuel driven emergency generators, which need testing. The emissions from testing these generators weekly may exceed those from the rare operation of a fossil fuel driven peak heating system.
When sizing electrical systems, we should be conscious of the diverse nature of energy loads in the building. We know that peak cooling load and peak heating load will not occur at the same time. And the data on consumption loads shows that not all outlets and lights will operate simultaneously. So, we shouldn’t oversize our electrical systems for conditions that do not exist.
Rather than electrify for the extremes, it makes more sense to design for normal, day-to-day operations and size the systems, the transformers, the switch gear, and the emergency generators appropriately. This approach is cost effective, it’s maintainable, and the space required is manageable. This means on the coldest day of the year, when extra heat is required, we turn to a fossil fuel source such as natural gas for that extra top up. We believe that some brief, limited carbon emissions when energy demand spikes are preferable to expensive and overdesigned electrical systems.
In this era of decarbonization by electrification, we are considering electrical demand as a design parameter of higher importance than before. And our first line of defense is efficiency and conservation.
We can make energy efficient design choices—using highly filtered recirculated air rather than 100 percent outdoor air, for example. It requires less energy. We can leverage high performing heat pump technologies. Once we have designed the facility to be as efficient as possible then we look at designing with technology to shift the demand peak. For example, by using geo-exchange or thermal energy storage we can store energy when it is either cheap to produce or we have a surplus of waste energy. Then the building can use it when demand is high.
We are responsible to make sure clients are aware of the costs and complexities associated with electrification and that they’re budgeted into the life cycle of the building. We can help the client forecast its electrical bill.
And through smart design, we minimize unwelcome surprises and extra costs.
To avoid the high arc flash hazard issue, for example, we can install the electrical distribution system with multiple panels, controls, and coordination to stagger activation of systems to avoid a rush of current. That way we can manage the need for specialty PPE and facilities training.
The goal is nearly fully electrified hospitals. It will still take years of planning and coordination with utilities to ensure sufficient generation and transmission capacity to support them.
In healthcare design, we always design for worst-case scenarios, what we sometimes call “Sharknado events.” That’s because hospitals are essential.
Many clients are asking us to design to 2080 climactic conditions. These clients are investing money now to get systems that will handle worst case climate scenario 40 or 50 years from now.
We need to remind clients that they’re going to replace this equipment decades before we reach those 2080 climatic conditions. It’s likely better to wait and install new, right-sized equipment later. That’s when we can see how climate change mitigation and electrification have played out.
We recommend they future proof through strategic decision making. They can use a modular design that allows them to expand later. We can size energy infrastructure for today’s demand plus some additional capacity and redundancy with the ability to expand that system in the future.
For example, we can make sure the pipes and the ducts above the ceilings and behind the walls are big enough to carry all the chilled water and air they will ever need. These are expensive to replace, so planning makes sense. We can make space for larger chillers. But for today, let’s install the right chillers to handle the next 25 years.
Some places, like Ontario, now require a carbon transition plan as part of a new hospitals design. It walks through a series of thought exercises (“do you have room in your existing building for new electrical supply?”) that can be helpful in planning for the electrified future and making the right decisions today.
All these thoughts are part of an important conversation about what we are going to electrify and when. We believe that with elegance and thoughtfulness we can electrify healthcare facilities sensibly, avoid unintended consequences, and set clients on the right path to a zero-carbon future.
In healthcare, every dollar saved can be put toward patient care, healthcare professionals, and space. So, some very modest carbon emissions are one way to balance capital and operational spending in this time of energy transition.


